
ACL Graft Options: Choosing The Graft That Works Best For You
What are ACL Injuries?
ACL injuries can be tough, so having a good medical team to help you along the way makes a big difference. Part of that process involves choosing which graft to utilize to replace the torn anterior cruciate ligament (ACL). Your orthopedic surgeon / sports medicine doc will take the time to discuss your options with you, but we believe in patient-centered care (meaning you should be an active participant in the decision making process). There are many options available, and the choice can seem overwhelming- so we here at Sarrica Physical Therapy & Wellness are here to help guide you in your decision making process!
Types of ACL Grafts
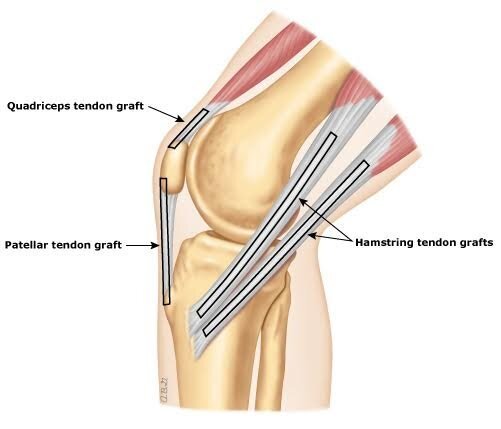
There are 2 different types of ACL grafts: autograft and allograft. An autograft is a tendon that is harvested from your own body and an allograft is harvested from a human cadaver. This is the first decision you need to make- autograft or allograft? Autografts are harvested from your patellar tendon, hamstring tendon, or quadriceps tendon. Allografts are most commonly from the patellar tendon, Achilles, or hamstring tendon of a human cadaver.
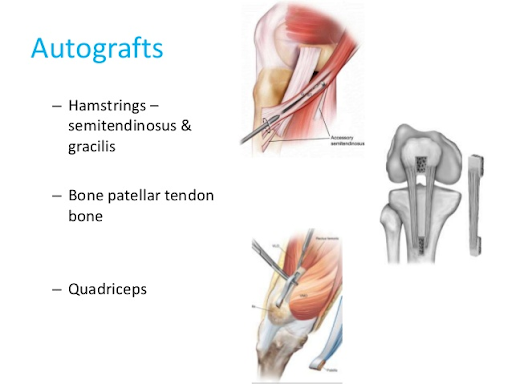
Autograft
An autograft tends to “take better,” meaning it develops a better fixation (it is absorbed better by the bones). The autograft has a significantly decreased failure rate compared to an allograft. The allograft is more likely to re-rupture and require ACL revision surgery. Competitive or recreational athletes in their teens, 20’s and 30’s should almost always consider an autograft, especially if it is their primary injury. The more active you are, the more likely you are going to strain that graft- especially if you participate in change of speed and change of direction sports/activities. If this is your situation, we suggest going with the autograft.
However, an autograft does require your surgeon to harvest your own tendon(s). This will result in more postoperative swelling and pain, and a more difficult time regaining strength and range of motion after surgery. Keep that in mind as you rehabilitate post-op.
If you do decide to go with an autograft, the next decision is which one! The 2 main options are as follows:
Bone-patellar tendon-bone (BPTB):
BPTB involves the patella bone, patellar tendon, and the tibial tubercle of the tibia (shin bone). This autograft has a great fixation and takes best. The research is mixed, but there is evidence that the failure rate of this autograft is better than that of the hamstring autograft. Young, female athletes should get the BPTB autograft. I most often recommend this autograft to a patient who I know wants to remain very active, and highly competitive in his/her sport.
Pros: strong fixation, best for preventing ligament/joint laxity, lower failure/retear rates
Cons: anterior knee pain, pain with kneeling, numbness/tingling/lack of sensation in the front of the knee, longer recovery time and return to sport (RTS)
Hamstring:
This type involves the semitendinosus and gracilis tendons of the hamstring. Although the research is mixed, it does seem like the rate of failure/retear is slightly higher with this autograft. The benefit is that there is often less pain and swelling associated with this autograft, and therefore a smoother recovery. Younger, active adults are most appropriate for this autograft. You can be a recreational athlete, but proceed with caution if you are a high level athlete that participates in sports that involve a lot of cutting and change of direction. Remember that by harvesting your hamstring tendons, you are sacrificing a lot of hamstring strength. One theory is that ACL injuries may occur due to a poor strength ratio between the quadriceps and the hamstrings. If you remove the hamstring tendons, this could further disrupt the strength ratio and lead to increased risk of retearing.
Pros: less postoperative pain and swelling, faster recovery and (RTS)
Cons: greater chance of joint laxity, possibly greater risk of failure/retear, hamstring muscle weakness and disrupted quad:hamstring strength ratio
Allograft
So, you may ask: why consider an allograft? An allograft does not require your surgeon to harvest your own tendon(s) as an ACL replacement. As a result, you will have less pain and swelling postoperatively. You also will have all of your original tendons intact, therefore there should not be as much weakness in a specific set of muscles postoperatively. In theory, this leads to a more smooth recovery. However, an allograft will not ultimately be as strong and durable as an autograft. Middle aged and older adults who are fairly sedentary, or live active lifestyles that don’t involve competitive/recreational sports should consider an allograft. Be aware that the rate of failure for allografts for those who participate in sports is significantly higher than for those who utilize autographs.
Summary
ACL reconstruction surgery involves a rigorous and labor intensive recovery. You will heal with time and quality physical therapy treatment. It is important to note that patients with ACL ruptures have an increased risk of developing knee osteoarthritis in the future. It is absolutely crucial that you rehabilitate the right way and remain diligent throughout the process. ACL rehab takes 6 months - 1 year. It can be grueling, but we will help you to persevere. We will be guiding you along the way, and you will be back to what you love before you know it!
We hope we have made your decision about ACL reconstruction and graft options a bit easier. If you have any additional questions or concerns about your upcoming surgery, please feel free to call us at 347-560-6920 or email us at paul@sarricapt.com.
Dr. Paul Nasri, PT, DPT
Doctor of Physical Therapy
Sarrica Physical Therapy & Wellness
Staff Physical Therapist